by Dr. Joel S. Hirschhorn
Americans who have taken COVID vaccine shots and those who have refused to capitulate to the coercion and propaganda are ill-informed about blood clots. This article provides summaries of key recently published research on two types of observed blood clots – microscopic and relatively large size – that merit serious attention and concern.
One inevitable conclusion is that the FDA with support from big media is not doing its job to ensure truly informed consent by those taking vaccine shots.
Canadian physician reports high levels of clots
Dr Charles Hoffe has been practicing medicine for 28 years in a small, rural town in British Columbia, Canada, and recently gave a long interview. He has given about 900 doses of the Moderna experimental mRNA vaccine to his patients. So, contrary to some critics, he is no anti-vaccine doctor.
The core problem he has seen are microscopic clots in his patients’ tiniest capillaries. He said “Blood clots occurring at a capillary level. This has never before been seen. This is not a rare disease. This is an absolutely new phenomenon.”
Most importantly, he has emphasized these micro-clots are too small to show up on CT scans, MRI, and other conventional tests, such as angiograms, and can only be detected using the D-dimer blood test. Using the latter, he found that 62% of his patients injected with an mRNA shot are positive for clotting. He has explained what is happening in bodies.
The spike proteins in the vaccine become “part of the cell wall of your vascular endothelium. This means that these cells which line your blood vessels, which are supposed to be smooth so that your blood flows smoothly now have these little spikey bits sticking out. … when the platelet comes through the capillary it suddenly hits all these COVID spikes and it becomes absolutely inevitable that blood clots will form to block that vessel.”
He made an important distinction: “The blood clots we hear about which the media claim are very rare are the big blood clots which are the ones that cause strokes and show up on CT scans, MRI, etc. The clots I’m talking about are microscopic and too small to find on any scan. They can thus only be detected using the D-dimer test…The most alarming part of this is that there are some parts of the body like the brain, spinal cord, heart and lungs which cannot re-generate. When those tissues are damaged by blood clots they are permanently damaged.”
This is his pessimistic, scientific view: “blood vessels in their lungs are now blocked up. In turn, this causes the heart to need to work harder to try to keep up against a much greater resistance trying to get the blood through your lungs. This is called pulmonary artery hypertension – high blood pressure in the lungs because the blood simply cannot get through effectively. People with this condition usually die of heart failure within a few short years.”
All these medical views have been suppressed by big media., but it was covered well in another alternative news site. And the doctor got some attention by submitting an open letter to the provincial Ministry of Health. A key point in that is this: “It must be emphasised, that these people were not sick people, being treated for some devastating disease.
These were previously healthy people, who were offered an experimental therapy, with unknown long-term side-effects, to protect them against an illness that has the same mortality rate as the flu. Sadly, their lives have now been ruined.”
The concept of micro blood clots has also been invoked for the serious impacts of COVID itself. The eminent Dr. Peter McCullough noted “So, this is a very different type of blood clotting that we would see with major blood clots in the arteries and veins. For instance, blood clots involved in stroke and heart attack.
Blood clots involved in major blood vessels in the legs. This was a different type of clotting and in fact the Italians courageously did some autopsies and found micro blood clots in the lungs. And so, we understood in the end, the reason why the lungs fail is not because the virus is there. It is because micro blood clots are there. … When People can’t breathe, the problem is micro-blood clotting in the lungs. …The spicule on the ball of the of the virus itself which damages blood vessels that causes blood clotting.” He has also openly stated that none of the COVID vaccines are safe for most people at little risk from COVID.
If spike protein is the cause of micro blood clots in COVID it is also reasonable to see the same phenomenon in vaccinated people impregnated with spike proteins, as Dr. Hoffe as explained.
As to the Canadian situation, The Public Health Agency of Canada (PHAC) in July estimated the rate of vaccine-related blood clotting in Canadians who have received the AstraZeneca vaccine and said there have been 27 confirmed cases to date in Canada, with five deaths among those cases, a rather high death rate.
But this is consistent with 6 out of 28 blood clot cases reported by Yale University for the J&J vaccine in the US Also noted was that these were a particularly rare and dangerous blood clot in the brain, known as cerebral venous sinus thrombosis (CVST), because it appears in the brain’s venous sinuses Also noted that there were abnormally low platelet levels in their blood, an unusual situation also found for those impacted by the AstraZeneca vaccine.
Wall Street Journal and Nature Journal
To its credit, the Wall Street Journal published a long article in July on the COVID vaccine blood clot issue. Here are highlights from it.
“Canadian researchers say they have pinpointed a handful of amino acids targeted by key antibodies in the blood of some people who received the AstraZeneca Covid-19 vaccine, offering fresh clues to what causes rare blood clots associated with the shot.”
“The peer-reviewed findings, by a team of researchers from McMaster University in Ontario, were published …by the science journal Nature. They could help doctors rapidly test for and treat the unusual clotting, arising from an immune-driven mix of coagulation and loss of platelets that stop bleeding.”
“The blood clotting, which some scientists have named vaccine-induced immune thrombotic thrombocytopenia, or VITT, has also been linked to Johnson & Johnson’s Covid-19 shot, though incidents have occurred less frequently with that shot than with AstraZeneca.”
“Though rare, the condition has proven deadly in more than 170 adults post-vaccination in the U.K., Europe and U.S., according to government tallies. Many were younger adults who appeared healthy before vaccination, researchers and drug regulators say.”
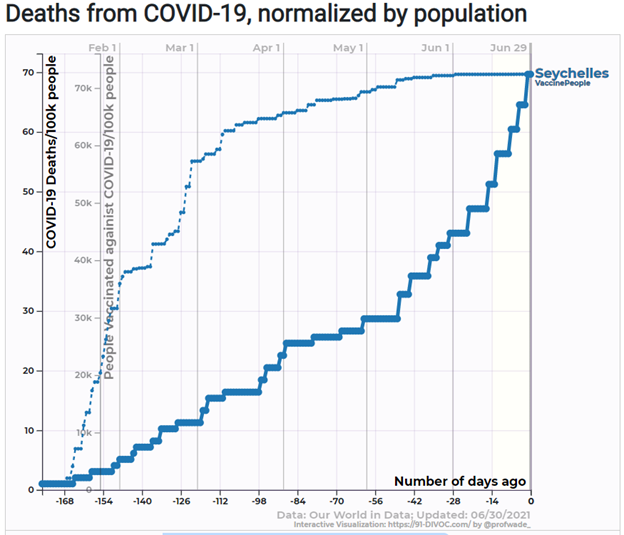
“The total number of cases after first or second doses in the U.K. was 395 through June 23…Of the 395, 70 people have died. European officials said this month that they have seen 479 potential cases of VITT out of 51.4 million AstraZeneca vaccinations…Far fewer potential cases—21 …followed J&J vaccinations in Europe. Of those cases, 100 deaths occurred after AstraZeneca vaccination and four after Johnson & Johnson, European regulators said.”
“U.S. health officials said in late June that they have identified 38 confirmed cases of the blood-clotting syndrome out of more than 12.3 million people who received the J&J vaccine…The Centers for Disease Control and Prevention said in May that three cases had been fatal and evidence ‘suggests a plausible causal association’ between the combination of low platelets and clotting and the vaccine.”
As to what is going on inside the body: “[In] rare cases, vaccinated people have experienced an autoimmune reaction in which antibodies bind with unusual strength to a blood component called platelet factor 4, or PF4, forming distinct clusters resembling a bunch of grapes. This so-called immune complex, a molecular formation in the blood, activates more platelets, ‘like putting a match to gasoline,’ said John Kelton, an author of the Nature paper and researcher at McMaster University.
The process accelerates, he and other researchers say, triggering simultaneous bleeding and clotting, sometimes in the brain, stomach and other areas that can in rare cases be deadly. ‘We think these antibodies are incredible amplifiers, in a bad way, of the normal coagulation system,’ says Dr. Kelton.”
Interestingly, this article did not mention at all the previously discussed case of the Canadian doctor and his findings about microscopic blood clotting.
New York Times
In April, there was limited coverage of stoppages of some vaccines: “First it was AstraZeneca. Now Johnson & Johnson. Last week, British regulators and the European Union’s medical agency said they had established a possible link between AstraZeneca’s Covid-19 vaccine and very rare, though sometimes fatal, blood clots.
The pause in the use of Johnson & Johnson’s vaccine in Europe over similar concerns threatens to hurt a sluggish rollout that was just starting to gain momentum.” Also noted was that states paused use of the J&J vaccine after a US advisory.
“Regulators have asked vaccine recipients and doctors to look out for certain symptoms, including severe and persistent headaches and tiny blood spots under the skin.”
New England Journal of Medicine
In April this journal published three research articles on blood clotting related to COVID vaccines and a long editorial by two physicians reviewing all the work. Here are highlights from the latter.
“The Journal has now highlighted three independent descriptions of 39 persons with a newly described syndrome characterized by thrombosis and thrombocytopenia that developed 5 to 24 days after initial vaccination with [the AstraZeneca vaccine]. … These persons were healthy or in medically stable condition, and very few were known to have had previous thrombosis or a preexisting prothrombotic condition.
Most of the patients included in these reports were women younger than 50 years of age, some of whom were receiving estrogen-replacement therapy or oral contraceptives. A remarkably high percentage of the patients had thromboses at unusual sites — specifically, cerebral venous sinus thrombosis or thrombosis in the portal, splanchnic, or hepatic veins. Other patients presented with deep venous thrombi, pulmonary emboli, or acute arterial thromboses. … High levels of d-dimers and low levels of fibrinogen were common and suggest systemic activation of coagulation. Approximately 40% of the patients died, some from ischemic brain injury, superimposed hemorrhage, or both conditions, often after anticoagulation.”
“Better understanding of how the vaccine induces these platelet-activating antibodies might also provide insight into the duration of antigen exposure and the risk of reoccurrence of thrombosis, which will inform the need for extended anticoagulation and might lead to improvements in vaccine design.”
“Additional cases have now been reported to the European Medicines Agency, including at least 169 possible cases of cerebral venous sinus thrombosis and 53 possible cases of splanchnic vein thrombosis among 34 million recipients of the [AstraZeneca] vaccine, 35 possible cases of central nervous system thrombosis among 54 million recipients of the Pfizer–BioNTech mRNA vaccine, and 5 possible (but unvetted) cases of cerebral venous sinus thrombosis among 4 million recipients of the Moderna mRNA vaccine. Six possible cases of cerebral venous sinus thrombosis (with or without splanchnic vein thrombosis) have been reported among the more than 7 million recipients of the Johnson & Johnson/Janssen vaccine.”
Here is the final conclusion; “The questions of whether certain populations can be identified as more suitable candidates for one or another vaccine and who and how to monitor for this rare potential complication will require additional study.”
Salk Institute
In April, the Salk Institute promoted coverage of research conducted by a number of people associated with it. The chief finding was that the spike protein associated with the COVID virus and with vaccines was connected to strokes, heart attacks and blood clots.
“The paper, published in Circulation Research, also shows conclusively that COVID-19 is a vascular disease, demonstrating exactly how the SARS-CoV-2 virus damages and attacks the vascular system on a cellular level. … the paper provides clear confirmation and a detailed explanation of the mechanism through which the [spike] protein damages vascular cells.”
A subsequent article in May examined this work and made several important observations. Here is its perspective, as relevant to the COVID vaccines. “The prestigious Salk Institute…has authored and published the bombshell scientific study revealing that the SARS-CoV-2 spike protein used in the Covid jabs is what’s actually causing vascular damage. Critically, all three of the experimental Covid vaccines currently under emergency use authorisation in the UK either inject patients with the spike protein or, via mRNA technology, instruct the patient’s own body to manufacture the spike protein and release them into the blood system.”
“The Salk Institute study proves the assumption made by the vaccine industry, that the spike protein is inert and harmless, to be false and dangerously inaccurate.”
“The research proves that the Covid vaccines are capable of inducing vascular disease and directly causing injuries and deaths stemming to blood clots and other vascular reactions. This is all caused by the spike protein that’s engineered into the vaccines.”
Report by 57 Medical Experts
This May report was prepared by nearly five dozen highly respected doctors, scientists, and public policy experts from across the globe. It went public and was urgently sent to world leaders as well as all who are associated with the production and distribution of the various Covid-19 vaccines in circulation today. The report demanded an immediate stop to COVID vaccinations. Dr. McCullough was one of the signatories.
“Despite calls for caution, the risks of SARS-CoV-2 vaccination have been minimized or ignored by health organizations and government authorities,” said the experts.
On the issue of blood clotting in vaccinated people the report said this:
“Some adverse reactions, including blood-clotting disorders, have already been reported in healthy and young vaccinated people. These cases led to the suspension or cancellation of the use of adenoviral vectorized [AstraZeneca] and [J&J] vaccines in some countries. It has now been proposed that vaccination with ChAdOx1-nCov-19 can result in immune thrombotic thrombocytopenia (VITT) mediated by platelet-activating antibodies against Platelet factor-4, which clinically mimics autoimmune heparin-induced thrombocytopenia.
Unfortunately, the risk was overlooked when authorizing these vaccines, although adenovirus-induced thrombocytopenia has been known for more than a decade, and has been a consistent event with adenoviral vectors. The risk of VITT would presumably be higher in those already at risk of blood clots, including women who use oral contraceptives, making it imperative for clinicians to advise their patients accordingly.”
Conclusions
Supporters of the COVID vaccines are quick to emphasize that relatively few recipients have experienced post-vaccination blood clotting. True, except for the findings of the Canadian physician about microscopic blood clots in most of his patients that major news media have ignored. Also ignored are the findings from the Salk Institute which provide a rationale for seeing spike proteins as causing clots. Even vaccines not directly including spike proteins – the AstraZeneca and J&J adenovirus vector vaccines – pose a problem because they send genetic instructions into cells to produce the spike protein of the coronavirus.
Even a June case study of one patient who died from clotting after taking the second dose of the Moderna vaccine and not related to anything else stressed the use of “safe” COVID vaccines. This was also stressed in an accompanying editorial that mentioned: “The highest reported incidence is 5 cases among about 130,000 Norwegian recipients of the [AstraZeneca] vaccine.”
This statistical view of the medical establishment was expressed as: “any potential risks of vaccination must be interpreted in the context of the overall morbidity and mortality of COVID-19 itself.” It also stressed blood clots in hospitalized COVID patients. It cannot be emphasized enough that the vast majority of COVID victims could have been saved through early home/outpatient treatment as detailed in Pandemic Blunder. The proven treatments can stop COVID infection in its early virus replication phase and, therefore, prevent blood clots.
The public also needs strong information about the many advantages of natural immunity, from prior COVID infection or life exposure to various coronaviruses. This is far better than vaccine induced artificial immunity that does less to protect against COVID variants and makes people susceptible to breakthrough infections. For most people the benefits of COVID vaccination do not outweigh the risks.
On the issue of whether all COVID vaccines pose a blood clot threat consider an April study by Oxford University that found the number of people who receive blood clots after getting vaccinated with a coronavirus vaccine are about the same for those who get Pfizer and Moderna vaccines as they are for the AstraZeneca vaccine. And as already cited the J&J vaccine has also been implicated for clots.
What needs attention by FDA, CDC and NIH is the need to do more testing of vaccine victims to discover through blood testing or autopsies the nature and extent of blood clotting.
For those wanting to see many examples of COVID vaccine negative health impacts this website is recommended. The mission is: “This website is dedicated to sharing the truth about these people and their testimonials. Watch for yourself and make up your own mind. Is it worth it to risk life-changing and even fatal side effects from a vaccine for a disease that is survived by 99.98% of people under 70?”
Of course, the risk of getting serious blood clots is much higher for those who get a serious case COVID-19 then it is for those who get vaccinated. They tend to be acute, near-term impacts amenable to various treatments, though sadly not lifesaving in all cases.
More insidious, in the longer run, however, perhaps years after the shots, are the microscopic blood clots noted by Dr. Hoffe and Dr. McCollough that may impact the lives of many people, perhaps millions.
Dr. Joel S. Hirschhorn, author of Pandemic Blunder and many articles on the pandemic, worked on health issues for decades. As a full professor at the University of Wisconsin, Madison, he directed a medical research program between the colleges of engineering and medicine. As a senior official at the Congressional Office of Technology Assessment and the National Governors Association, he directed major studies on health-related subjects; he testified at over 50 US Senate and House hearings and authored hundreds of articles and op-ed articles in major newspapers. He has served as an executive volunteer at a major hospital for more than 10 years. He is a member of the Association of American Physicians and Surgeons, and America’s Frontline Doctors.