
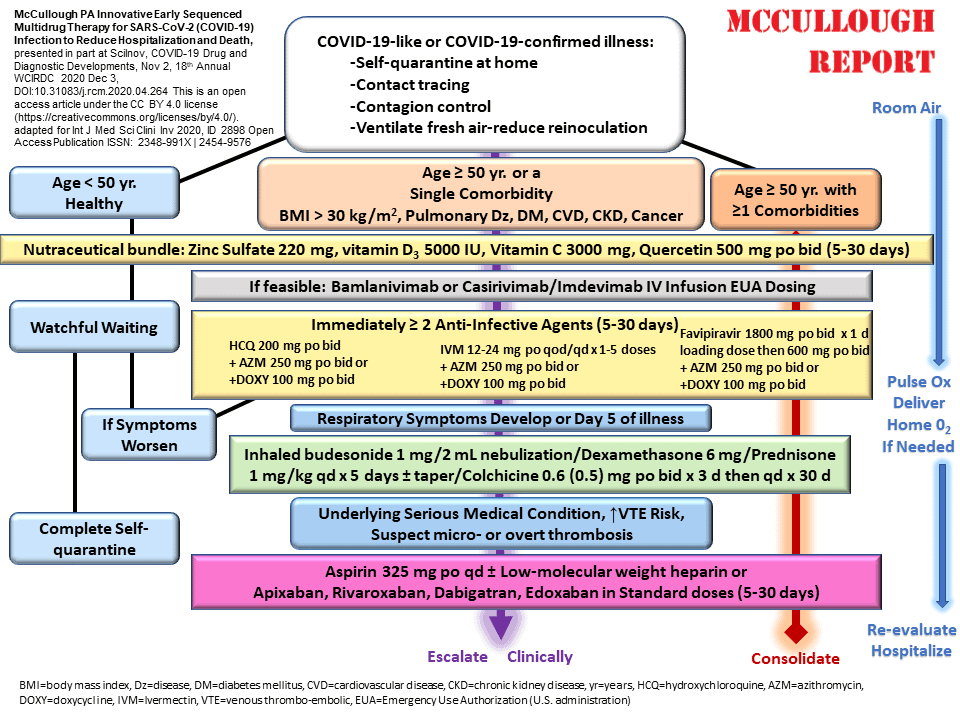
It is important to understand that COVID-19 always starts out with mild symptoms, so don’t make the mistake of assuming a “mild” case and ignoring early treatment. Take the approach that COVID-19 will be a short mild upper respiratory infection with prompt early therapy.
There is a list of over-the-counter nutraceuticals and aspirin that all households should have in stock to be ready. For the prescription drugs, a doctor will need to call these orders into a pharmacy, and this can be done by your doctor if they are willing and capable, and if not, by national or regional telemedicine services.
The links below give the key websites for you to access to get treatment guides and access telemedicine services. Do this early since outbreaks tend to jam up these services. Many have learned that early at-home treatment gives more effective medications than the hospital offers. The goal is to get as many days of multidrug home treatment before throwing in the towel for the hospital. If things worsen usually driven by extreme difficulty in breathing, a trip to the emergency room should be considered.
Patients are encouraged to take their home medications into the hospital and continue them since in-hospital care is commonly minimal and has a major focus on giving oxygen and mechanical ventilation. The National Institutes of Health Guidelines, which are strictly followed by most hospitals, do not advise treatment until a patient requires oxygen, this means that some patients go days in the hospital with no therapy.
That is the reason why it is so important to pack up home medications and take them to the hospital in the rare case treatment at home fails. Once in the emergency room, seniors should demand a monoclonal antibody infusion before release to home or admission. These lifesaving treatments are available to outpatients only, and sadly, once admitted to the hospital they are not offered in the current nihilistic approach to COVID-19 hospitalized care.
The most important drugs in the hospital are blood thinners and patients should demand full dose blood thinners (enoxaparin injections or heparin infusions) and adult aspirin. These are not offered to many patients and when COVID-19 deaths occur in the hospital the most common finding is blood clots in the lungs and elsewhere in the body due to inadequate anticoagulation. Hopefully with these tips, for those who have COVID-19 or will get it soon, whether vaccinated or not, will be useful in keeping the syndrome to a mild 4-day cold and a deliverance to natural immunity which reigns superior over the failed attempts at vaccine protection.
The monologue of this McCullough Report kicks off with a segment from an interview with Sebastian Gorka, Ph.D., who himself received successful early treatment and then moves into a detailed step by step approach of what should be done for children with serious background medical problems or presenting with severe symptoms and all adults over age 50 particularly the elderly and those with background medical problems.
This week’s show features Dr. Chris Montoya, Ph.D., who is a research professor of psychology and “brain science” at Thompson Rivers University in Kamloops British Columbia, Canada. I’ve asked him to help us understand the mass psychosis that is occurring where doctors are in a trance, brainwashed into not treating COVID-19, losing empathy, and then without concern over safety or efficacy, are blindly promoting the failed mass vaccination program. His insights are terrific.
So, let’s get real, let’s get loud, on America Out Loud Talk Radio, this is The McCullough Report!
The McCullough Report: Sat/Sun 2 PM ET Encore 7 PM – Internationally recognized Dr. Peter A. McCullough, known for his iconic views on the state of medical truth in America and around the globe, pierces through the thin veil of mainstream media stories that skirt the major issues and provide no tractable basis for durable insight. Listen on iHeart Radio, our world-class media player, or our free apps on Apple, Android, or Alexa.









{kind=link}